New noninvasive RNA tests could help identify at-risk pregnancies

For expectant parents, pregnancy can be a time filled with joyful anticipation: hearing the beating of a tiny heart, watching the fetus wiggling through the black-and-white blur of an ultrasound, feeling the jostling of a little being in the belly as it swells.
But for many, pregnancy also comes with serious health issues that can endanger both parent and child. In May, for example, US Olympic sprinter Tori Bowie died while in labor in her eighth month of pregnancy. Potential factors contributing to her death included complications of preeclampsia, a pregnancy-specific disorder associated with high blood pressure. Preeclampsia occurs in an estimated 4.6 percent of pregnancies globally. Left untreated, it can lead to serious problems such as seizures, coma and organ damage.
Both preeclampsia and preterm birth are relatively common conditions that can put both the mother and her baby at risk of health issues both before and after birth. But doctors don’t have a good way to determine whether an individual will develop one of these complications, says Thomas McElrath, an obstetrician-gynecologist at Brigham and Women’s Hospital in Boston. Currently, physicians primarily look to a woman’s prior pregnancies, medical history and factors such as age and ethnicity to determine her risk. These measures are useful, but limited, and may fail to identify problems early enough to enable effective treatment, McElrath says. “They’re not as precise as I think most of us, as clinicians, would really want.”
That may soon change. Scientists are learning that free-floating bits of genetic material found in a pregnant person’s blood may offer a way to detect complications such as preeclampsia and preterm birth — although some experts caution that it’s too early to determine how useful these tests will be in the clinic. In the meantime, the tests are providing researchers with a new way to unravel the underlying biology of these inscrutable ailments.
Risk predictions
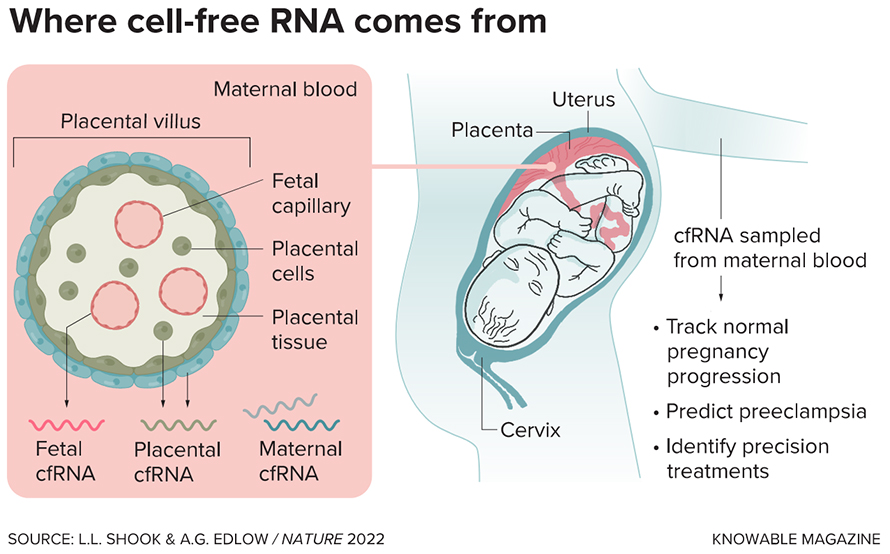
All of us carry bits of our own genetic material — both DNA and its more evanescent cousin, RNA — around in our bloodstreams. During pregnancy, these free-floating fragments, known as cell-free DNA and RNA, are also released from the developing fetus into the mother’s blood, primarily via the placenta, which contains cells from both parent and child. For more than a decade, clinicians have used cell-free DNA from blood to screen the fetus for genetic abnormalities.
But DNA provides a largely static view of the genetic content within our cells. RNA, on the other hand, gives a snapshot of which genes are turned on or off at a specific point in time. Since gene activity varies across cells and over time, researchers realized that they could use RNA to glean a more dynamic view of the changes that occur within the mother’s body during pregnancy. RNA enables scientists to look beyond the fixed genotype to factors that change over the course of pregnancy such as prenatal complications, says Mira Moufarrej, a postdoctoral researcher at Stanford University who coauthored a paper in the 2023 Annual Review of Biomedical Data Science on noninvasive prenatal testing with RNA and DNA.
To screen for possible complications, scientists have been looking at cell-free RNA in pregnant women’s blood that originates from both mother and child. Some of the earliest studies of this kind emerged in the early 2000s. In 2003, for example, Dennis Lo, a chemical pathologist at the Chinese University of Hong Kong, and his colleagues reported that in a study of 22 pregnant women, a specific RNA found in the placenta was much more abundant during the third trimester in those who had preeclampsia than in those who did not. Over the years, Lo’s group and others have looked at broader changes in RNA during pregnancy in larger groups of people.
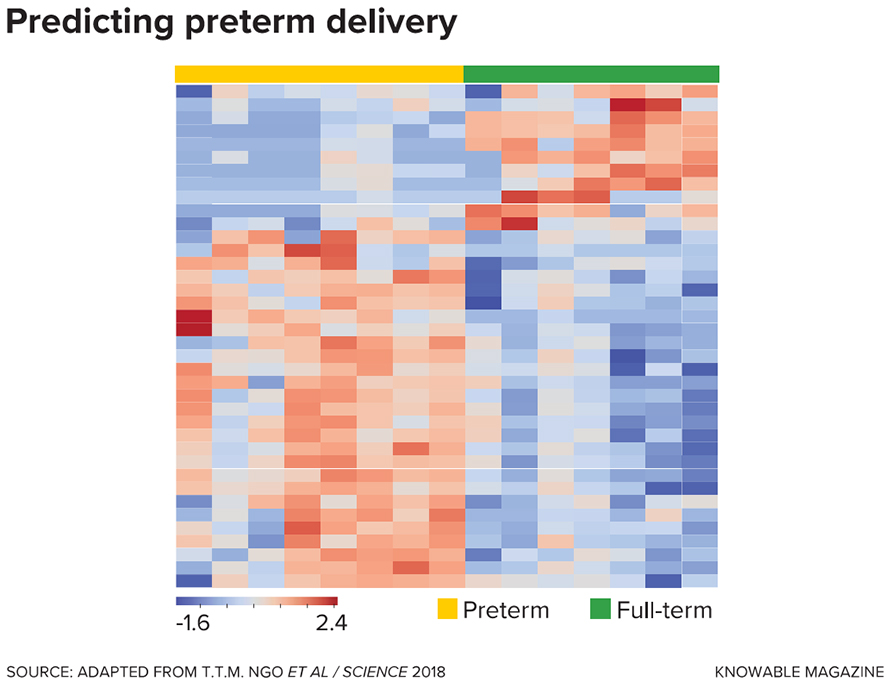
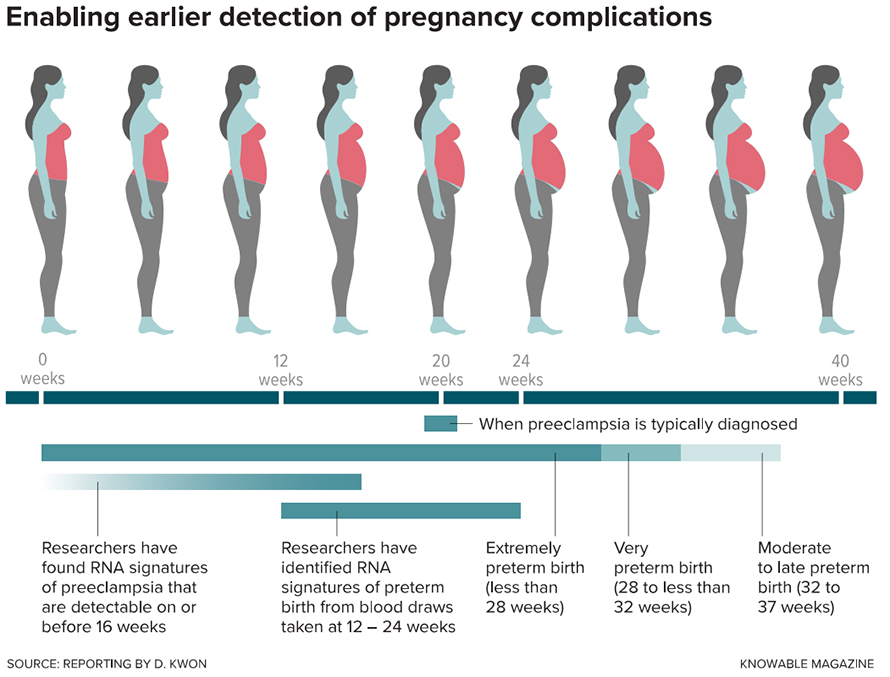
In a 2018 study, Moufarrej, who was then a doctoral student, her advisor Stephen Quake, a biophysicist at Stanford University, and colleagues reported that cell-free RNA could help determine when labor would occur. The researchers recruited 38 pregnant women in the United States known to be at risk of preterm birth, and then drew a blood sample from each in either the second or third trimester. By comparing cell-free RNA in those who eventually delivered prematurely to those who gave birth at full term, they were able to identify a set of RNAs that appeared up to two months prior to labor that could pinpoint around 80 percent of premature births.
That proof-of-concept investigation spurred the researchers to look further and examine whether cell-free RNA could also predict preeclampsia. Other groups had previously reported RNA-based signatures of preeclampsia — in 2020, for instance, scientists working with the California-based biotech company Illumina reported dozens of RNA transcripts that were unique to pregnant women with the condition. But Moufarrej, Quake and their colleagues wanted to track RNA changes throughout pregnancy to see whether it might be possible identify people at risk of preeclampsia during early pregnancy, before symptoms began.
In a study published in 2022, the researchers recruited 73 mothers at heightened risk of preeclampsia and drew blood from them four times: at or before 12 weeks, between 13 and 20 weeks, at or after 23 weeks, and after birth. Afterward, the researchers compared cell-free RNA for the 24 women who indeed developed preeclampsia against the remaining 49 who did not. The team identified RNAs corresponding to 544 genes whose activity differed in those who developed preeclampsia and those who did not. (The study did not differentiate between maternal and fetal RNA, but since the majority of cell-free RNA in a pregnant person’s blood is their own, Moufarrej says most of these RNAs are likely maternal in origin.)
Then, using a computer algorithm, the researchers developed a test based on 18 genes that could be used prior to 16 weeks of pregnancy to predict a woman’s risk of developing preeclampsia months later. The test correctly identified all the women who would later develop preeclampsia — and, equally important, all of the women who the test predicted wouldn’t develop preeclampsia did in fact escape the disease. (About a quarter of the women predicted to develop preeclampsia did not, in fact, get the disease.) The same 18-gene panel also correctly predicted most cases of preeclampsia in another group of 118 women.
The team also took a closer look at which tissues the RNA of interest originated from. This included the usual suspects, such as the lining of the blood vessels (also known as the endothelium), which scientists already know contributes to preeclampsia, as well as other, more unexpected sources, such as the nervous and muscular systems. The authors note that, in the future, this information could be used both to understand how preeclampsia affects different parts of the body and to assess which organs are at highest risk of damage in a particular patient.
According to Quake, studies like these from both his team and others are starting to reveal the diversity of changes throughout the body that contribute to pregnancy complications — and providing evidence for something that clinicians and researchers have long suspected: that both preeclampsia and preterm birth are conditions with a range of underlying causes and outcomes. “There are now strong indications that you should be defining multiple subtypes of preeclampsia and preterm birth with molecular signatures,” says Quake. “That could really transform the way physicians approach the disease.”
Research teams elsewhere are also looking at other pregnancy complications such as reduced fetal growth, which can cause infants to be at higher risk of problems such as low blood sugar and a reduced ability to fight infections. Some of these tests are now being validated in large, multicenter studies, while others are still in the early days of development.
The road to the clinic
RNA-based tests for both preeclampsia and preterm birth risk are inching their way toward the clinic. Mirvie, a company cofounded by Quake in South San Francisco, is focused on developing both. Last year, the company published a study of a preterm birth test with hundreds of pregnant individuals as well as one on a preeclampsia test with thousands of participants. Both studies boasted promising results. The company is now in the middle of an even larger study of the preeclampsia test that will include 10,000 pregnancies, Quake says. (Quake and Moufarrej are both shareholders of Mirvie.)
Cell-free RNA-based tests for preeclampsia are leading the way, says McElrath, likely because preterm birth has more subtypes and more potential causes — including carrying multiples, chronic health conditions such as diabetes, and preeclampsia — which make it a more complicated issue to address. (McElrath is involved in validating Mirvie’s tests; he serves on its scientific advisory board and has a financial stake in the company.)
Still, questions about these tests remain. An important next step, says Moufarrej, is determining what’s behind the RNA changes associated with a heightened risk for these pregnancy complications. All the studies conducted to date have been correlative — linking patterns in RNA with risk — but to provide effective treatment, it will be important to determine the cause of these changes, she adds. Another open question is how important maternal versus fetal RNAs are to determining the risk of pregnancy complications. To date, most studies have not distinguished between these two sources. “This remains an active area of investigation,” McElrath says.
Erik Sistermans, a human geneticist at Amsterdam UMC in the Netherlands, says that while there is a lot that researchers can learn from cell-free RNA, it’s still too early to judge what the power of these RNA-based tests will be in clinical practice. He notes that he and other researchers are also investigating the possibility of using cell-free DNA to determine the risk of pregnancy complications like preeclampsia. For example, some groups are looking at chemical modifications to DNA known as epigenetic changes, which occur in response to age, environment and other factors.
Yalda Afshar, a maternal fetal medicine physician at the University of California, Los Angeles, agrees that it’s still unclear whether these tests will provide benefits not available from existing screening methods such as looking for the presence of risk factors. For these screening tests to truly benefit patients, clinicians will first need to understand the underlying biology of these complications — and have effective treatments to offer patients found to be at risk, she adds. (Afshar is an unpaid consultant for Mirvie.)
There are also ethical questions to consider. Screening tests provide only an estimate of risk, not a definitive diagnosis, Sistermans notes. Before these tests are rolled out to the public, it will be critical to consider how best to communicate test results, and what next steps to take for individuals who are identified as being in a high-risk category, he says. For preeclampsia, low-dose aspirin can help prevent or delay its onset, while the hormone progesterone may help prevent some cases of preterm birth. Still, every additional test added to a prenatal screen makes decisions more complicated and potentially stressful for pregnant women. “You shouldn’t underestimate the amount of anxiety these kinds of tests may cause,” Sistermans says.
Still, researchers are optimistic about the future of cell-free RNA-based tests. The tests for preeclampsia are already more accurate than currently available tests for the condition, according to McElrath. And if researchers succeed in predicting other complications, he adds, future patients will benefit not just from additional information about their pregnancies, but also from the opportunity to receive more personalized care. “Once we start to see success in early preeclampsia prediction,” McElrath says, “it will quickly spread out from there.”
Editor’s note: This story was updated August 25, 2023, to to clarify the results of a study on predicting preeclampsia from RNA in the mother’s blood. The original version stated that the test correctly identified 85 percent of preeclampsia cases. In fact, the test correctly identified all preeclampsia cases, but about a quarter of positive test results were women who did not go on to develop preeclampsia.
This article originally appeared in Knowable Magazine, an independent journalistic endeavor from Annual Reviews.
Enjoy reading ASBMB Today?
Become a member to receive the print edition four times a year and the digital edition monthly.
Learn moreGet the latest from ASBMB Today
Enter your email address, and we’ll send you a weekly email with recent articles, interviews and more.
Latest in Science
Science highlights or most popular articles

Glaucoma model links immune signaling to disease progression
Researchers at Duke University determine genetic variations that could increase the risk of developing glaucoma.

Uncovering the molecular roots of fatty liver disease
Physician–scientist Silvia Sookoian discusses her path from hepatitis C care to MASLD research, her use of multi-omics to study steatotic liver disease, and how lipid metabolism and genetics are reshaping understanding of MASH and liver health.
Mitochondria shape kidney cell function
Researchers at the University of Washington, Seattle present the first quantitative comparison of mitochondrial interactomes between two epithelial cell types in the kidney.

Long-chain polyunsaturated fatty acids linked to postoperative delirium risk
Researchers show that altered lipid metabolism may contribute to postoperative delirium, a condition linked to increased risk for long-term cognitive decline. The study explores potential disease mechanisms, which have yet to be understood.

Glycosylation patterns across antibody isotypes distinguish tuberculosis states
Researchers at Taipei Medical University present the first site-specific glycosylation analysis of immunoglobulins in elderly tuberculosis patients.
Blood glycome possibly predicts lifespan
Researchers at the University of Santiago de Compostela show that total serum N-glycome can predict mortality independent of traditional risk factors.